Fluid Documentation Should Be as Fast as Speaking.
Nurses work with gloved hands, moving between rooms, managing multiple patients. The keyboard is the bottleneck. BedSync’s voice layer lets nurses log fluid events the moment they happen — tap, speak, confirm.
Natural Language Parsing
Say it naturally: “240 mL cranberry juice”. BedSync’s NLP engine extracts fluid type, volume, and route, then maps cranberry juice to its water equivalent automatically. Select the patient, tap the mic, speak, confirm. No rigid commands. No memorized syntax.
Structured Data, Not Free Text
Voice input doesn’t create a free-text note. It populates discrete, structured fields: volume, fluid type, route (oral/IV/output), and timestamp. Running balance updates instantly. Data is export-ready as FHIR R4 or CSV for your EHR.
Three Input Modes
Voice, barcode scanning, and manual entry — each optimized for a different workflow. Scan an IV bag for instant product lookup, speak a bedside observation, or tap through quick-log buttons. Every entry is verified on-screen before it commits.
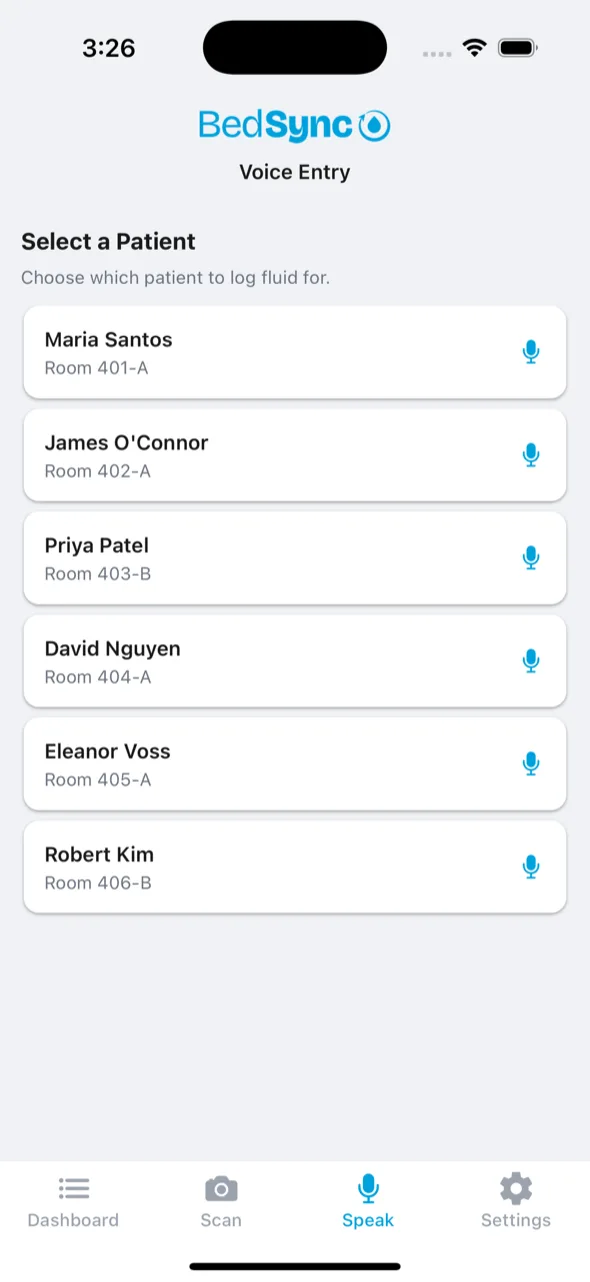
Context-Aware Patient Selection
Open from a patient’s chart and voice is pre-assigned. Open from the ward view and BedSync shows a quick patient picker. Tap a name, tap the mic, done. The system auto-detects intake vs. output from natural speech.
No one else is applying voice intelligence to fluid balance. Dragon Copilot, Commure, and Aiva handle general nursing documentation. BedSync is the only platform combining voice capture with fluid-specific NLP, I/O conversion logic, and AKI risk staging.



